
Interoperability for Patient Data is Here. Is Your Leadership Ready?
- Jason Hatfield

- Jan 8
- 4 min read
A Pragmatic Disruptor’s Guide to the New Dawn of Connected Healthcare

The headlines are buzzing: OpenAI has officially entered the healthcare arena with ChatGPT Health.
By partnering with b.well Connected Health to tap into FHIR-based APIs, they’ve effectively turned the "digital front door" into a conversational reality. Patients can now connect their medical records, wearables, and wellness apps to a single AI interface.
For the consumer, it’s a new dawn of clarity. For the Product Manager, it’s the ultimate test of Grounded Leadership.
As a Pragmatic Disruptor™, I see this as a tectonic shift in the Architecture of Potential. People are already using Gemini, Copilot, and ChatGPT to navigate their health journeys, investment plans, and careers—but in the healthcare space, they have been doing it at their own risk because the data was not in a closed loop. With OpenAI’s recent announcement, that loop is closing.
However, as product teams race to leverage this opportunity, we must step back. No one wants to be on the evening news for a data breach. Technology is no longer the hurdle—the hurdle is the Trust Commodity.
Connecting systems is the Disruptor move. Building the framework to protect that connection is the Pragmatic necessity.
The 10 Pragmatic Guardrails for Healthcare AI
To move beyond the "Build Trap" of simply connecting APIs, Product Leaders must enforce these 10 guardrails to truly Transform Outcomes.
The GIGO Filter: Connectivity without curation is a liability. Implement automated validation—if EMR data is fragmented or missing units of measure, the AI must flag "Insufficient Context" rather than hallucinating a trend.
The HIPAA/PII "Moat": Ensure a strict architectural boundary. While the LLM processes data to provide insights, it must never retain that data for foundation model training.
The Trust Commodity: Trust is a finite resource. One "creepy" or unprompted health suggestion can bankrupt a user’s confidence. In 2026, I believe that buying and selling Trust will become the core Value Proposition for high-performing product teams.
Regulatory Mirroring: The landscape is shifting. From the 21st Century Cures Act to state mandates like California’s AB 3030, your UX must include clear disclaimers that AI is not a diagnostic provider.
The "Uncertainty" Protocol: Program your AI to say, "I don't know, and..." and then explore the next steps the user wants to take. Inform the user when speculation arises. This becomes your gold mine for user feedback and risk acceptance.
Contextual Compartmentalization: Prevent "cross-chat leakage." You never want a request for a chocolate cake recipe to turn into advice on preventing pre-diabetes unless the user expressly asks for that correlation.
Bias & Equity Auditing: Regularly audit outputs to ensure advice isn't inadvertently discriminatory due to historic gaps in medical data (e.g., the 20% lower accuracy rates often seen in clinical algorithms for underrepresented groups). GIGO management is key.
The Human "Exit Ramp": Always provide a one-click path to a verified human provider or clinical source. AI should bridge the gap to a doctor, not replace the bridge.
Lineage & Auditability: Every insight must be traceable. Litigation will eventually stem from these interactions. Audit logs and fully compliant documentation retention are mandatory from Day 1—not an afterthought!
Incremental Activation: Don't flip the switch on a full longitudinal history on Day 1. Start with "Low-Risk" data (e.g., Pharmacy or Wellness) and expand as the model’s accuracy is proven in private POCs.
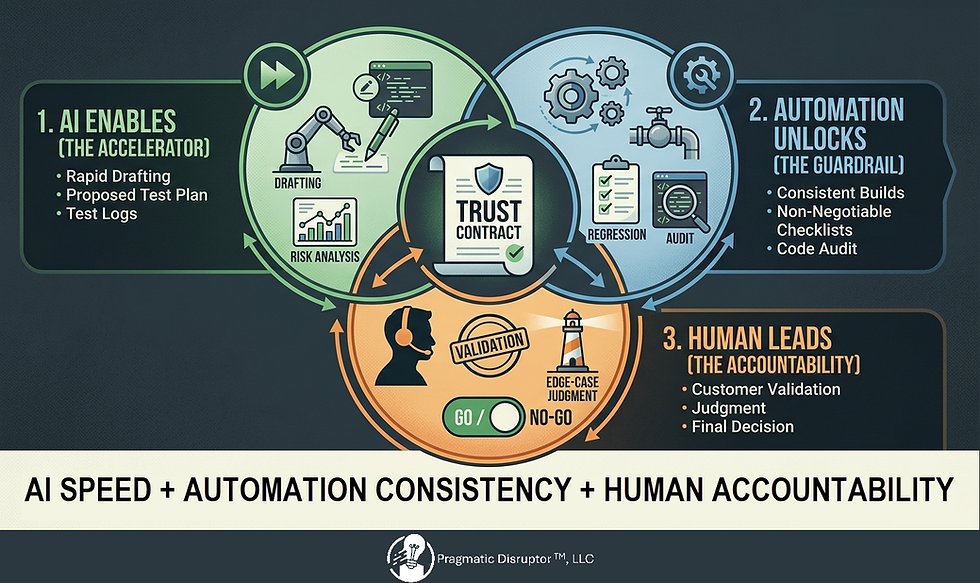
The Action Plan: Human in the Loop (HITL)
In my S.M.I.L.E. Paradigm, we "Empower Team Always." This means evolving the Product Owner from a "Story Writer" to an AI Agent Manager when the Agile team is building AI solutions.
Changes to the Squad Roles
AI Agent Manager: Governs the "System Prompt" and ensures AI logic aligns with product strategy.
Clinical Data Curator: An MD or RN who reviews "Gold Sets" of AI responses to ensure clinical safety.
Privacy Architect: Manages the data "Moat" and ensures compliance with information-blocking rules.
The Pragmatic Milestone Path
Phase 1: The Data Refinery. Cleanse and standardize EMR data via FHIR. Solve the GIGO problem at the source.
Phase 2: The "Quiet Dawn" (Private POC). Test the "Uncertainty Protocol" with internal clinicians to identify where the AI struggles.
Phase 3: Trust Commodity Audit. Conduct deep-dive user interviews. Does the connectivity feel empowering or invasive?
Phase 4: Restricted Beta. Open to 1,000 users for "Low-Risk" queries only (e.g., explaining lab terms).
Phase 5: Full Launch & Monitoring. Track the "Exit Ramp" usage. If users are jumping to humans, analyze if the AI is providing value or causing confusion.
The Pragmatic Disruptor Takeaway
The launch of ChatGPT Health is a reminder that high-performing teams aren’t built by accident—they are built through trust, intent, and shared ownership.
We have the tools to connect the fragmented world of healthcare. But as leaders, we must ask: Have we built the guardrails necessary to protect the person behind the data?
Disrupt the Norm | Transform Outcomes
Call to Action: Are you building connected health systems? What is your favorite "GIGO Guardrail" to enforce? Share your insights below—I’d love to learn from your journey.

Comments